


WHAT ARE CONTRAINDICATIONS TO TESTING?
These include severe uncontrolled hypertension, severe left ventricular hypertrophy, severe aortic stenosis and most importantly an inability to exercise.
HOW DOES IT FIT IN CLINICALLY?
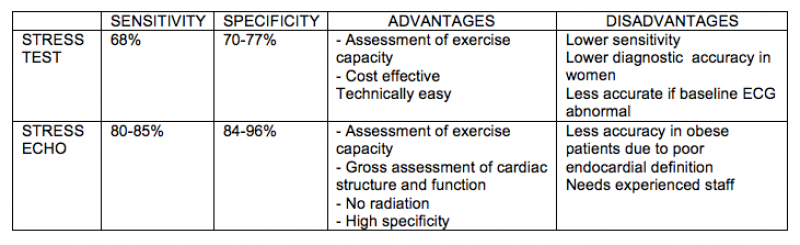
The tests are most accurate in patients with an intermediate pretest probability of CAD (10-90%). These are patients in whom the test will change risk stratification, ie: to low or high risk. The tests accuracy depends on the population being tested. In other words lower risk patients are more likely to yield a false positive result (eg: a 20 year old female with an abnormal stress test is likely to be a false positive). The higher the pre-test probability of CAD, the lower the risk of a false positive result (eg: a 65 year old diabetic smoker with an abnormal result will likely be true positive). A STRESS ECHO HAS LESS FALSE NEGATIVE AND FALSE POSITIVE RESULTS ACROSS THE SPECTRUM AND IS DEFINITELY BECOMING THE TEST OF CHOICE AMONGST CARDIOLOGISTS and GP’s. High risk patients with a good story for CAD should be considered for an angiogram. If there are any concerns, a pre-test consultation or chat with a cardiologist is advised.
DOES THE STRESS ECHO GIVE ME THE SAME INFO AS A STANDARD ECHOCARDIOGRAM?
Absolutely not. The stress echo only involves a brief interrogation of valves and cardiac structure but will not make a full assessment. If a full assessment of valves (for regurgitation and stenosis) is required, then a separate request for a transthoracic echocardiogram should me made. It is reasonable to ask for an echocardiogram as well as a stress echocardiogram/stress test.
WHAT DO I TELL MY PATIENT?
Before the stress test your patient will be connected to a 12-lead ECG and a baseline ECG recording will be performed. If undergoing a stress echocardiogram, a brief baseline echocardiogram will also be performed to assess the cardiac structure and function. The stress test involves walking on a treadmill. The treadmill will start on a low incline at a slow speed and will usually increase in incline or speed every 2–3 minutes. In stress echocardiography, a baseline echocardiogram is performed, and then the stress test is undertaken followed by an immediate post-stress echocardiogram. It is essential to take the post-stress images quickly as the heart rate usually recovers rapidly (the maximum time in the standard imaging protocol is only 90 seconds). The team performing the test will encourage the patient move rapidly from the treadmill to the bed for this reason. This can be more challenging for the elderly or anxious person and a stress test may be less intimidating in this case.
HOW DOES THE TEST WORK?
Cardiac stress testing works on the principle of demonstrating inducible ischaemia as workload increases (Stress ECG identifies ischaemia if horizontal or down-sloping ST depression of ≥1 mm at 80 m/sec after the J-point is induced with exercise.
Stress echocardiography assesses the ECG response to stress as well as obtaining an immediate poststress echocardiogram to assess for inducible wall motion abnormalities as a marker of ischaemia. The cardiologist will analyse the pre- and post-images to assess for alterations in wall motion based on a standard 17-wall segment model.
WHAT DO THE RESULTS MEAN?
The report should include an indication for the test. The results should describe the exercise protocol used, the exercise capacity in terms of time and workload achieved (protocol level, workload in watts or metabolic equivalent [METs] achieved), the haemodynamic response to stress (baseline and maximum blood pressure), at what heart rate and at what percentage of maximum heart rate the test was ceased, for what reason the test was ceased, presence of left ventricular hypertrophy or inducible ischaemia (in terms of ST segment shift or wall motion abnormalities on echocardiography), presence or absence of arrhythmia and heart rate response during recovery. The report may also comment on chronotropic incompetence and oxygen saturation during the test. Metabolic equivalent is a multiple of basal oxygen consumption, which is 3.5 mLO2/kg/min, and is the most robust assessment of exercise capacity as it is standard between the different forms of stress and protocols used. There is a very low risk of a cardiac event (<1% per year) if seven METs are achieved for men or five for women. A stress echocardiogram report may additionally comment on the effect of exercise on valvular function (eg. degree of stenosis or regurgitation), pulmonary pressure, inducibility of outflow tract gradients (obstruction) and cardiac shunting.
WHAT ARE THE NEXT STEPS?
Depending on the clinical scenario, a positive EST or ESE may be an indication for cardiology referral to consider coronary angiography or optimise medical therapy for coronary artery disease
WHAT ARE THE COSTS?
All investigations, including stress tests and stress echocardiograms are bulk billed at all Peninsula Cardiology clinics.